
Medically Reviewed
Last updated: 30/01/2025
Diabetic nephropathy, also known as diabetic kidney disease, is a serious complication of both type 1 and type 2 diabetes. Approximately one in three individuals with diabetes will develop diabetic nephropathy.
This condition impairs the kidneys’ normal function of eliminating waste products and excess fluids from the body. Maintaining a healthy lifestyle and properly managing diabetes and hypertension are the most effective ways to prevent or delay the onset of diabetic nephropathy.
Over time, this condition progressively damages the kidneys’ filtering units. Early intervention may help slow the progression or prevent complications.
Diabetic kidney disease can ultimately lead to kidney failure, also referred to as end-stage kidney disease (ESKD), which is life-threatening.
Symptoms
In the early stages, diabetic nephropathy may not present with any noticeable symptoms. As it advances, the following may occur:
- High blood pressure that becomes increasingly difficult to control
- Swelling in the feet, ankles, hands, or around the eyes
- Foamy urine
- Difficulty concentrating or confusion
- Shortness of breath
- Loss of appetite
- Nausea and vomiting
- Persistent itching
- Fatigue and weakness
When to consult a nephrologist
If you have symptoms of kidney disease, it is important to consult a nephrologist. Individuals with diabetes should undergo annual evaluations, or as frequently as recommended, to assess kidney function.
Causes
Diabetic nephropathy arises when diabetes damages the small blood vessels and cellular structures within the kidneys. The kidneys contain millions of microscopic filtering units called glomeruli, which remove waste from the bloodstream. Damage to these vessels impairs the kidneys’ ability to function and may result in kidney failure.
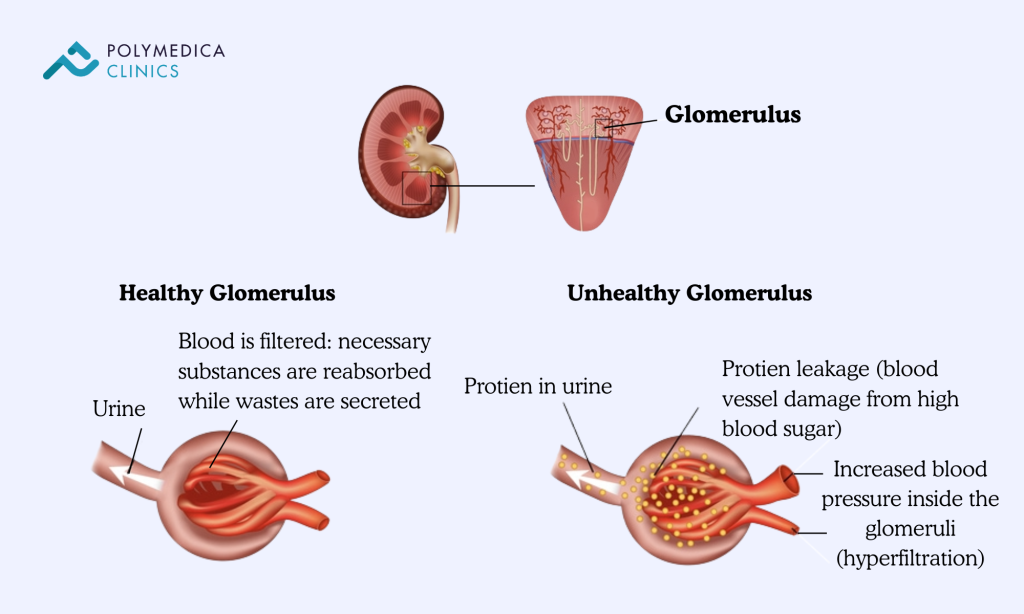
Uncontrolled diabetes causes blood vessel damage, while high blood pressure further exacerbates this by increasing pressure within the filtration system of the kidneys.
Risk Factors
For individuals with diabetes, the risk of diabetic nephropathy is increased by:
- Poorly managed blood glucose levels
- Poorly controlled hypertension
- Tobacco use
- Elevated blood cholesterol
- Obesity
- Family history of diabetes and kidney disease
Complications
Complications may develop gradually over months or years and include:
- Fluid retention, leading to limb swelling, hypertension, or pulmonary oedema
- Elevated potassium levels in the blood (hyperkalaemia)
- Cardiovascular disease, including increased risk of stroke
- Anaemia due to reduced red blood cell production
- Pregnancy complications affecting both mother and fetus
- Irreversible kidney damage resulting in end-stage kidney disease requiring dialysis or transplantation
Prevention
To reduce the risk of diabetic nephropathy:
- Visit your endocrinologist and nephrologist regularly to monitor diabetes and kidney function
- Maintain optimal blood glucose levels to slow or prevent kidney damage
- Effectively manage hypertension and other comorbidities with the guidance of your medical team
- Use over-the-counter medications, such as pain relievers, only as directed. Non-steroidal anti-inflammatory drugs (NSAIDs) like Ibuprofen (Brufen®) or Diclofenac (Cataflam®) can worsen kidney damage
- Achieve and maintain a healthy weight through regular physical activity
- Avoid smoking, as it accelerates kidney damage.
Diagnosis
Diabetic nephropathy is typically detected during routine monitoring for individuals with diabetes. Testing is recommended annually for those with type 2 diabetes or type 1 diabetes for more than five years.
Common screening tests include:
- Urinary albumin test: Detects the presence of albumin, a protein not typically found in urine if kidney function is normal
- Albumin-to-creatinine ratio (ACR): Assesses kidney function by comparing protein levels to creatinine in a urine sample
- Glomerular filtration rate (GFR): Calculated from blood creatinine levels to estimate kidney filtration efficiency
Additional diagnostic tests may include:
- Imaging: Ultrasound, X-rays, CT scans, or MRI to evaluate kidney structure and blood flow
- Kidney biopsy: A sample of kidney tissue is collected using a fine needle under local anaesthesia for microscopic analysis
Treatment
The initial focus in treating diabetic nephropathy is managing diabetes and blood pressure. This involves dietary changes, regular exercise, and prescribed medications. Stabilising glucose and blood pressure levels may prevent or delay kidney damage.
Medications may include:
- ACE inhibitors or ARBs to control blood pressure
- Blood glucose-lowering agents, such as insulin, metformin, SGLT2 inhibitors, or GLP-1 receptor agonists
- Statins to manage high cholesterol and reduce protein in the urine
- Finerenone to minimise kidney scarring and reduce the risk of kidney failure and cardiovascular complications
Regular monitoring is essential to assess disease progression and treatment effectiveness.
Management of advanced diabetic nephropathy
For individuals with kidney failure, treatment focuses on replacing lost kidney function or providing supportive care:
- Haemodialysis: A machine filters waste and fluid from the blood. This typically occurs three times weekly in a dialysis centre or at home with appropriate training. Each session lasts about 3 to 5 hours.
- Peritoneal dialysis: The peritoneum (abdominal lining) is used to filter waste using a special fluid. This can be done at home or work, though it’s not suitable for everyone.
- Kidney transplant: In some cases, a kidney or kidney-pancreas transplant may be the most appropriate option. A full evaluation will determine eligibility.
- Palliative care: For those who opt not to pursue dialysis or transplant, symptom-focused treatment is provided for comfort in the remaining months of life.
Potential future treatments
Research into regenerative medicine may offer future solutions to reverse or slow kidney damage. Techniques under investigation include pancreatic islet cell transplantation and stem cell therapy, which may improve kidney function if diabetes can be effectively cured or controlled through these methods.
Lifestyle and self-care
Long-term management requires attention to lifestyle factors, including:
- Blood sugar monitoring: Follow your endocrinologist’s advice on when and how often to check glucose levels.
- Physical activity: Engage in at least 150 minutes of moderate to vigorous aerobic exercise each week (e.g., walking, swimming, cycling).
- Nutrition: Consume a diet rich in fibre, fruits, non-starchy vegetables, legumes, and whole grains. Minimise intake of saturated fats, processed meats, sugars, and salt.
- Stop smoking: Seek support to quit smoking, which significantly worsens kidney and cardiovascular health.
- Weight management: Aim to achieve or maintain a healthy weight. If needed, discuss safe weight-loss strategies, including possible surgical options, with your specialist.
- Low-dose aspirin: Ask your cardiologist or endocrinologist whether you should take daily low-dose aspirin to reduce cardiovascular risk.
- Coordination of care: Ensure all your treating specialists are aware of your diabetic nephropathy diagnosis. They can modify treatment plans to avoid kidney-damaging procedures, such as contrast dye imaging (angiograms or CT scans).
This article is for informational purposes only and does not constitute a diagnosis or treatment, nor does it substitute professional medical advice.